BACKGROUND: Bovine respiratory syncytial virus (BRSV) is a major cause of respiratory disease in cattle worldwide. Calves are particularly affected, even with low to moderate levels of BRSV-specific maternally derived antibodies (MDA). Available BRSV vaccines have suboptimal efficacy in calves with MDA, and published infection models in this target group are lacking in clinical expression. Here, we refine and characterize such a model. RESULTS: In a first experiment, 2 groups of 3 calves with low levels of MDA were experimentally inoculated by inhalation of aerosolized BRSV, either: the Snook strain, passaged in gnotobiotic calves (BRSV-Snk), or isolate no. 9402022 Denmark, passaged in cell culture (BRSV-Dk). All calves developed clinical signs of respiratory disease and shed high titers of virus, but BRSV-Snk induced more severe disease, which was then reproduced in a second experiment in 5 calves with moderate levels of MDA. These 5 calves shed high titers of virus and developed severe clinical signs of disease and extensive macroscopic lung lesions (mean+/-SD, 48.3+/-12.0% of lung), with a pulmonary influx of inflammatory cells, characterized by interferon gamma secretion and a marked effect on lung function. CONCLUSIONS: We present a BRSV-infection model, with consistently high clinical expression in young calves with low to moderate levels of BRSV-specific MDA, that may prove useful in studies into disease pathogenesis, or evaluations of vaccines and antivirals. Additionally, refined tools to assess the outcome of BRSV infection are described, including passive measurement of lung function and a refined system to score clinical signs of disease. Using this cognate host calf model might also provide answers to elusive questions about human RSV (HRSV), a major cause of morbidity in children worldwide.
Excerpt from my doctoral defense presentation
In study III, we refined and characterized a BRSV challenge model in calves and a set of tools to evaluate challenge outcomes. This part of my project was a collaboration between three labs, in three different countries, and to facilitate study IV, as well as follow-up studies in the three labs, we needed a common challenge model. We wanted a challenge model with consistently high clinical expression, because unfortunately, without clinical signs in control calves which are similar to the upper spectrum of clinical signs observed in the field, you can’t conclude on the protective efficacy of vaccines.
In study III, 2 groups of 3 calves with low levels of specific maternal antibodies were challenged by aerosol inhalation of one of two virulent inocula: Either Snook strain BRSV passaged in calves (BRSV-Snk) or a Danish isolate passaged in cell culture (BRSV-Dk) After challenge, calves were monitored for seven days.
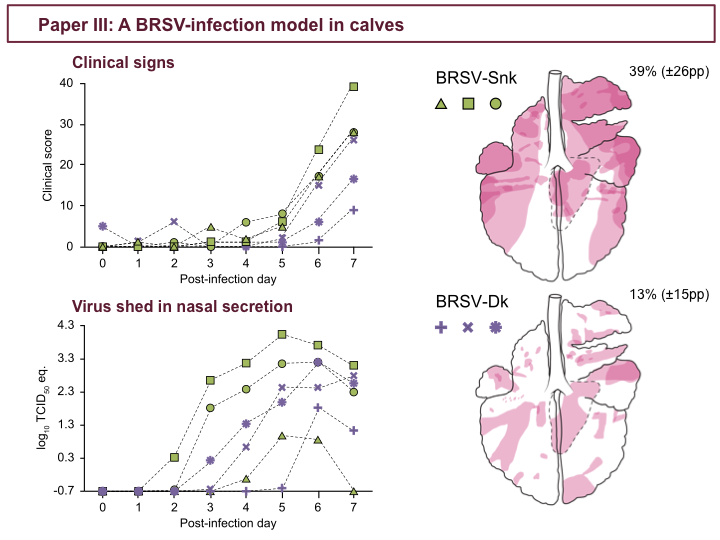
During those seven days all calves developed clinical signs of BRSV-infection, as illustrated by daily clinical scores in the upper figure. All calves also shed virus in nasal secretion, detected by quantitative PCR shown in the lower figure, and in BAL, which is not shown. Also, all calves had consolidative lesions in the lungs on post-infection day 7, as seen in these per-group superimposed lung charts. After challenge, one BRSV-Snk-calf demonstrated a rapid seroconversion and we determined that this calf had been previously exposed to BRSV. This is the calf with the green triangles, with less virus shed in nasal secretions, compared to the other BRSV-Snk calves. This calf is discussed further in the thesis. Nonetheless, overall BRSV-Snk-infected calves had more severe clinical signs on post-infection day 7, including general depression, reduced appetite and fever (with a mean peak rectal temperature of 40°C) and nasal discharge and coughing, abdominal dyspnea, wheezing and increased respiratory rate (with a mean peak respiratory rate of 87 breaths per minute), and except for the one calf, the remaining BRSV-Snk-infected calves shed more virus than calves infected with BRSV-Dk.
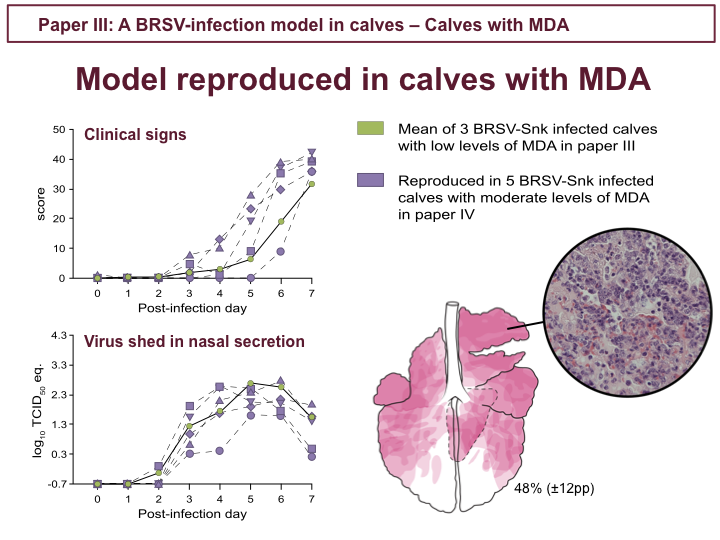
For the reasons mentioned in the previous figure, the BRSV-Snk inoculum were chosen for the challenge in study IV. Calves in study IV had moderate levels of specific serum MDA, and are descibed further in paper IV. This figure is just to show that unvaccinated controls in study IV, in purple, demonstrated similar clinical signs, virus shed and pathology to that which I described for BRSV-Snk-infected calves with low specific serum MDA, in green circles in these figures.
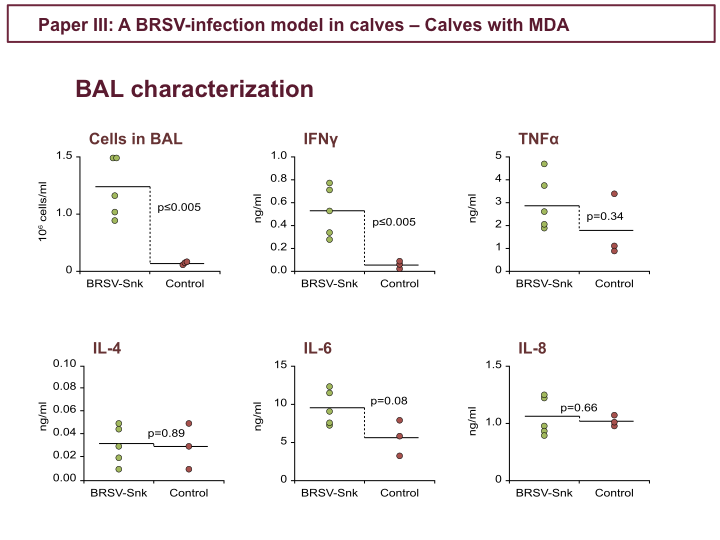
In study III, samples and data from the 5 calves with specific MDA in the previous figure were used to identify additional parameters which might be used to evaluate the efficacy of vaccines in future studies. For example, we investigated cell numbers in BAL samples collected on post-infection day 7 from these five calves, and compared to uninfected control calves these were significantly elevated, and consisted predominantly of neutrophils. Also, elevated levels of IFN gamma in BAL supernatant, which supports a viral infection. We also analyzed concentrations of other cytokines in BAL, as indicated in this figure. Cytokines which have previously been reported to be elevated during primary BRSV-infection, but we did not detect any significant differences, which may be due to suboptimal timing of BAL collection.
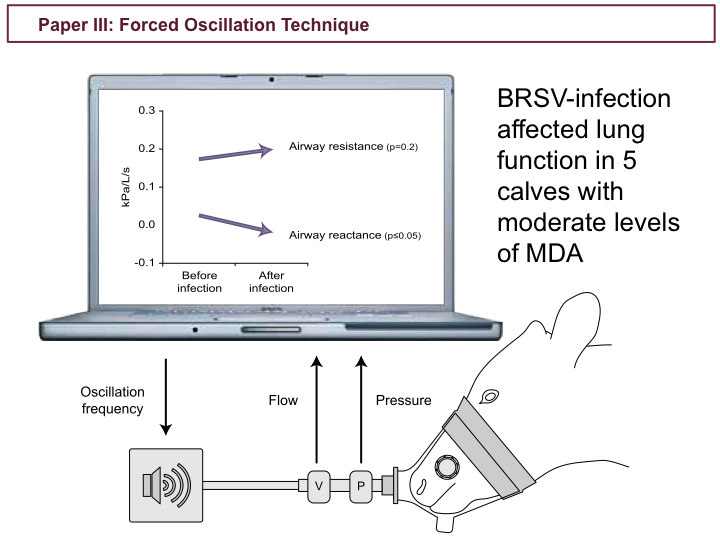
In study III, we also used the Forced Oscillation Technique (FOT) to passively measure lung function in the 5 calves with specific MDA, before and after challenge, as FOT might be used as an additional objective tools to measure the protective efficacy of vaccine candidates. FOT measures the flow and pressure at a given frequency of oscillation, and analyzes the resistance and reactance in the airways. Using FOT, we demonstrated that severe BRSV-infection in calves had a negative effect on lung function, with reduced airway reactance and a tendency of increased airway resistance. Although this method will need some optimization, I believe FOT could be a very useful tool in future BRSV vaccine evaluations.
To summarize our findings in study III, challenge by aerosol inhalation of the BRSV-Snk inoculum reproduced BRSV infection in calves with specific maternal antibodies, and this model can be used to evaluate the efficacy of vaccines and antivirals.
We now had the common methods and tools to reproducibly induce BRSV infection, and evaluate the efficacy of vaccines, in the three labs. This model was used in study IV.